Understanding Osteoporosis: Bone Density, Fracture Risk, and Treatment Options
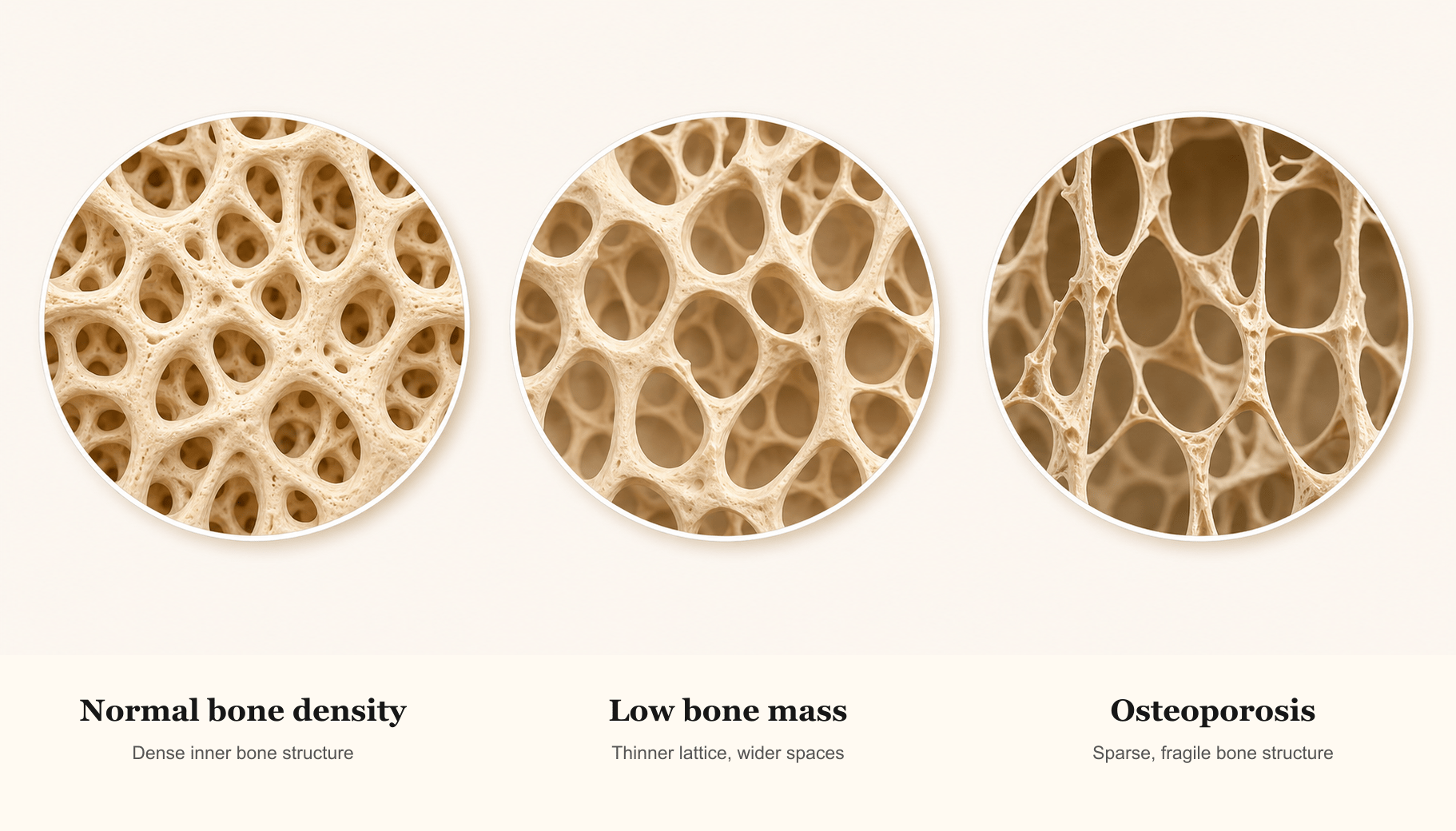
Osteoporosis is a condition in which bones become weak, thin, and fragile. Healthy bone is constantly being broken down and rebuilt. In osteoporosis, bone is broken down faster than it is rebuilt, leading to loss of bone mass and changes in bone structure that make fractures more likely.
Osteoporosis is sometimes called a silent disease because there are usually no symptoms until a fracture occurs. That is why bone density testing, fracture risk assessment, nutrition, movement, and treatment planning all matter.
This guide explains how osteoporosis is diagnosed, why untreated bone loss matters, what you can do to support bone health, and when medication may be recommended.
Quick Takeaways
- Osteoporosis is common and serious, but it is treatable.
- A DXA scan measures bone mineral density and reports a T-score.
- Nutrition, exercise, fall prevention, and medication decisions all matter.
- Never stop denosumab (Prolia) without a transition plan from your clinician.
What Is Osteoporosis?
Bone is living tissue. It is always being remodeled, with old bone removed and new bone formed. Osteoporosis develops when bone loss outpaces bone rebuilding.
The result is not just less bone, but weaker bone structure. That is why fractures can happen from a fall, a minor injury, or sometimes even ordinary daily activities.
Understanding T-scores
A DXA scan is a painless test that estimates bone mineral density. The result is reported as a T-score.
- Normal: -1.0 or above
- Osteopenia: between -1.0 and -2.5
- Osteoporosis: -2.5 or below
Why Untreated Osteoporosis Matters
Osteoporosis-related fractures can have a major impact on health, independence, and quality of life. Spine fractures may cause pain, height loss, or posture changes. Hip fractures can lead to hospitalization, long recovery, and loss of independence.
Fractures Can Be Major Health Events
The reason treatment matters is what can happen after a fracture. In women over 55, osteoporosis-related fractures are a major cause of hospitalization and have been reported to cause more hospitalizations than heart attack, stroke, and breast cancer combined. Hip fracture is the most serious osteoporosis complication: many studies report that about 1 in 4 older adults die within the first year after a hip fracture, and many survivors never return to their previous level of independence. Some require long-term nursing home care.
These comparisons are not meant to say every patient has the same risk, but they do show that osteoporosis deserves the same prevention mindset as blood pressure, cholesterol, diabetes, and cancer screening. Many osteoporosis treatments can substantially reduce fracture risk, with some lowering certain fracture risks by 50% or more. The goal is to prevent the first fracture when possible, and to prevent the next one when a fracture has already happened.
Fractures can occur with everyday activity and may increase the risk of more spine fractures.
Hip fractures are among the most serious complications and can threaten independence.
Other fractures can disrupt daily life and signal higher future fracture risk.
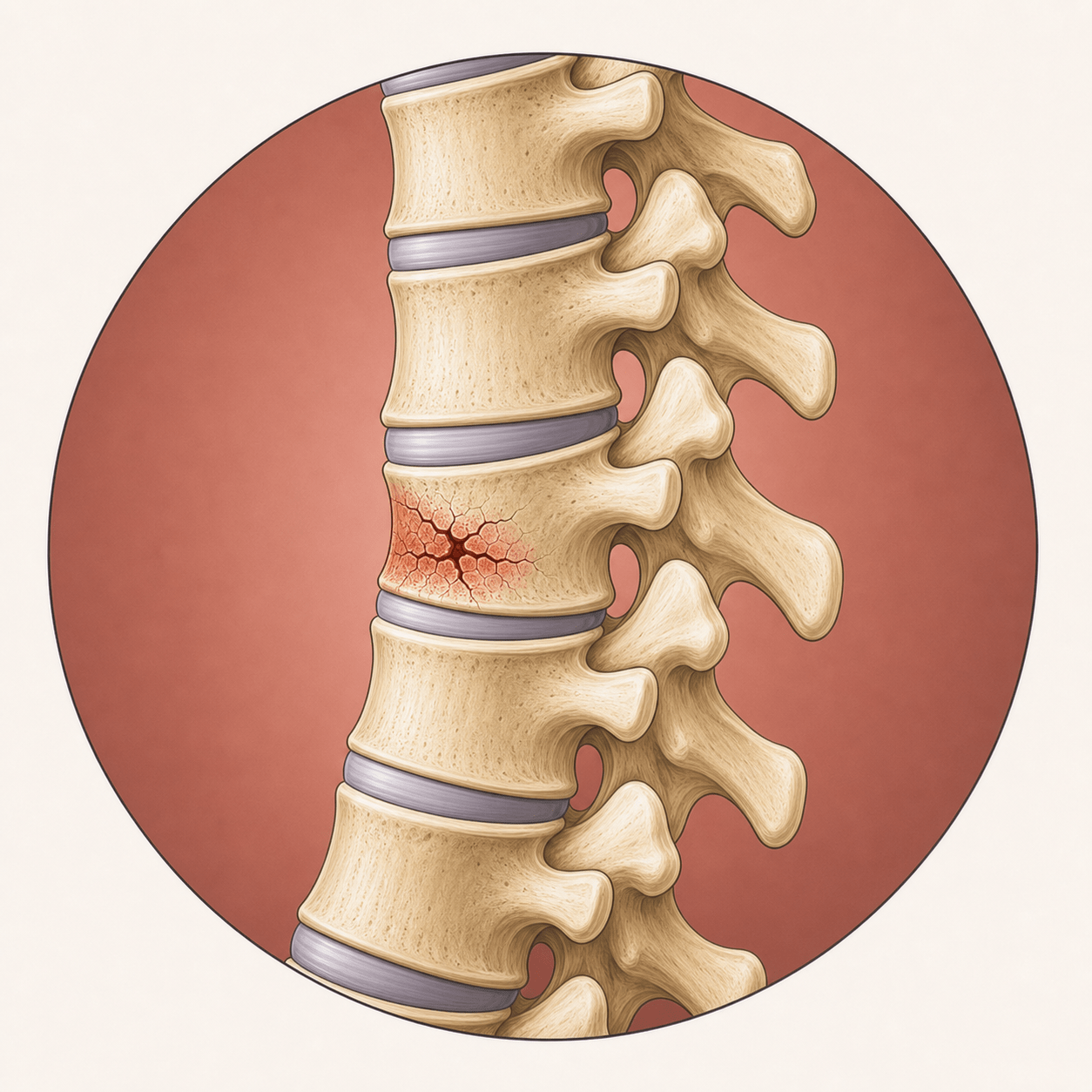 Spine
Back pain, height loss, or posture changes
Spine
Back pain, height loss, or posture changes
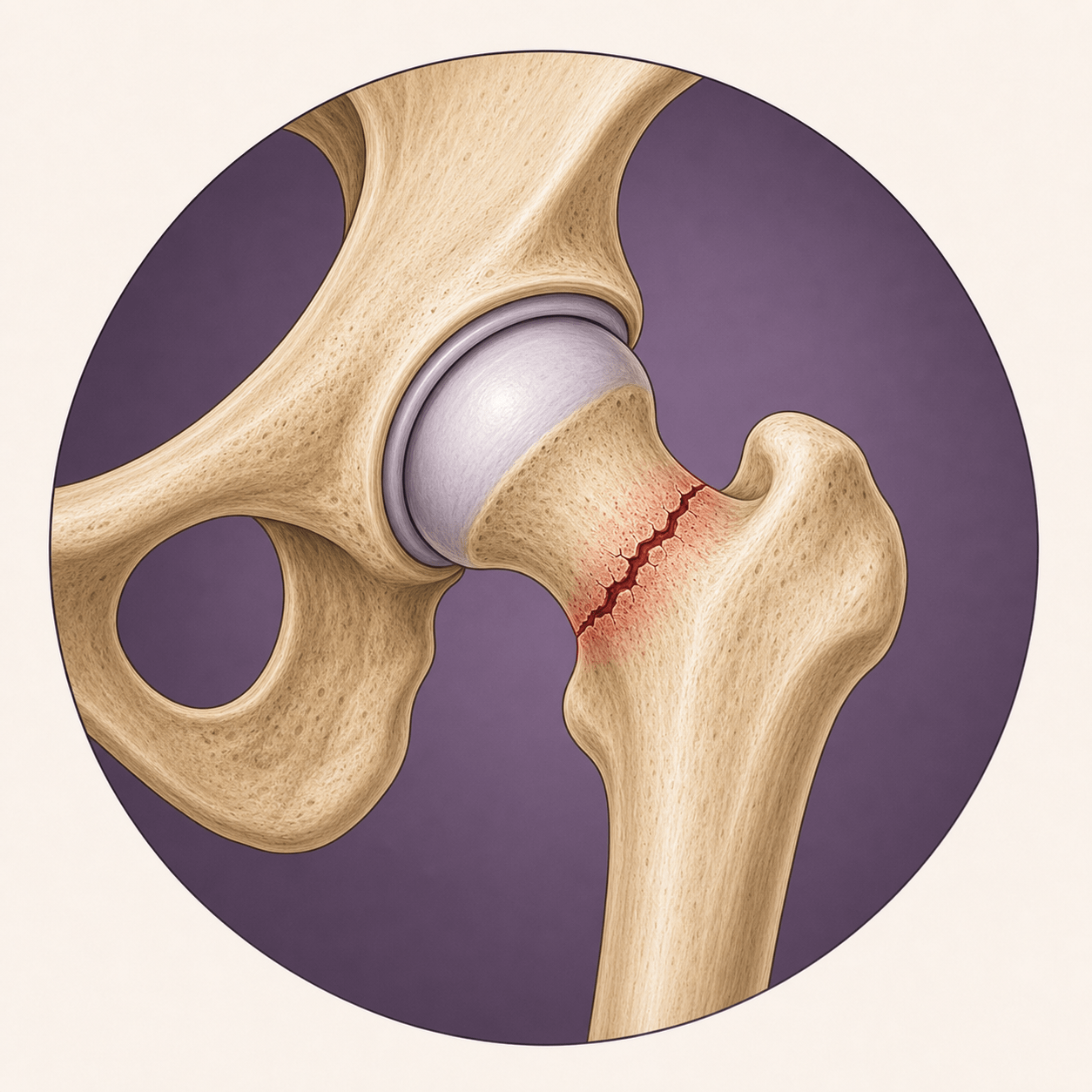 Hip
Often serious and can threaten independence
Hip
Often serious and can threaten independence
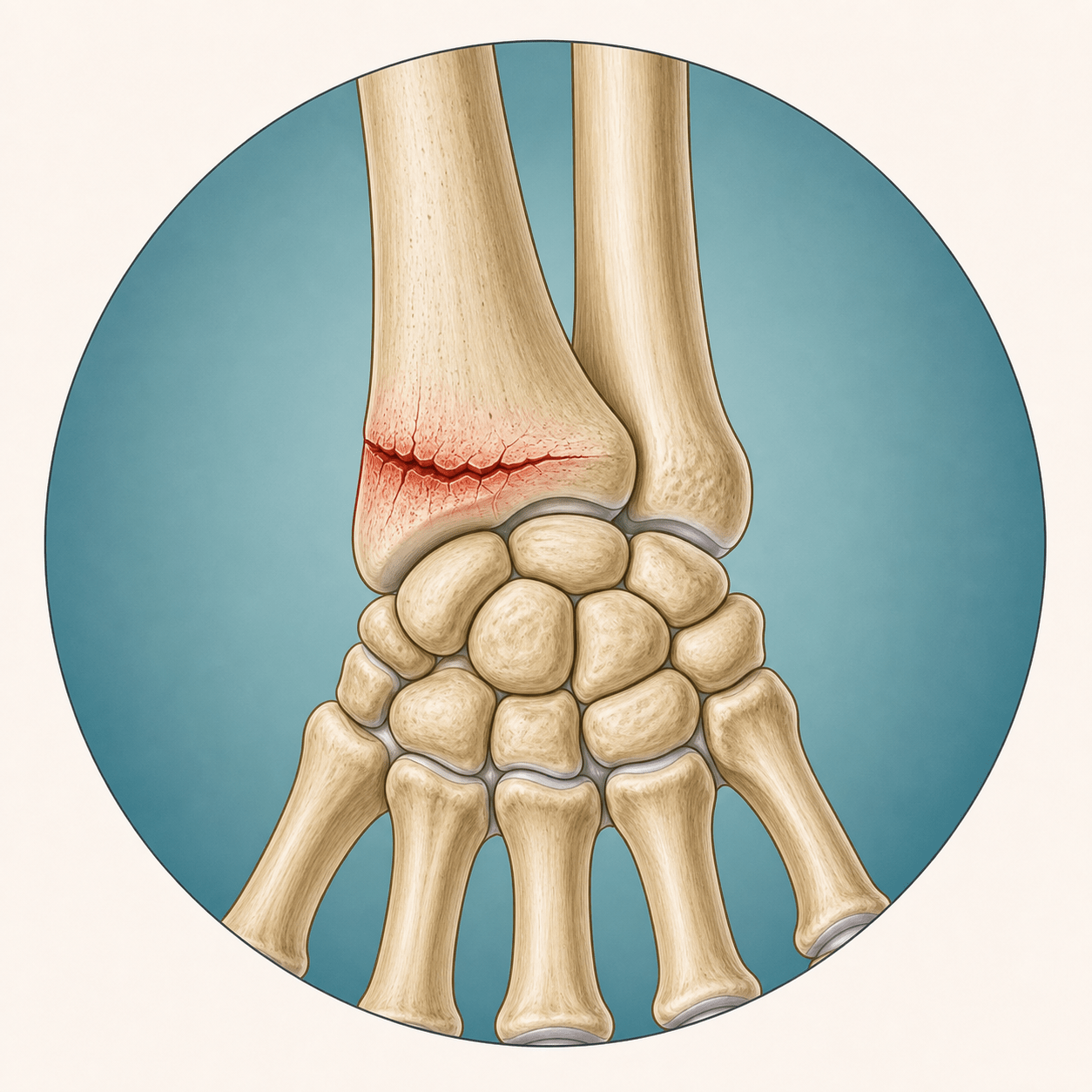 Wrist
Common after a fall onto an outstretched hand
Wrist
Common after a fall onto an outstretched hand
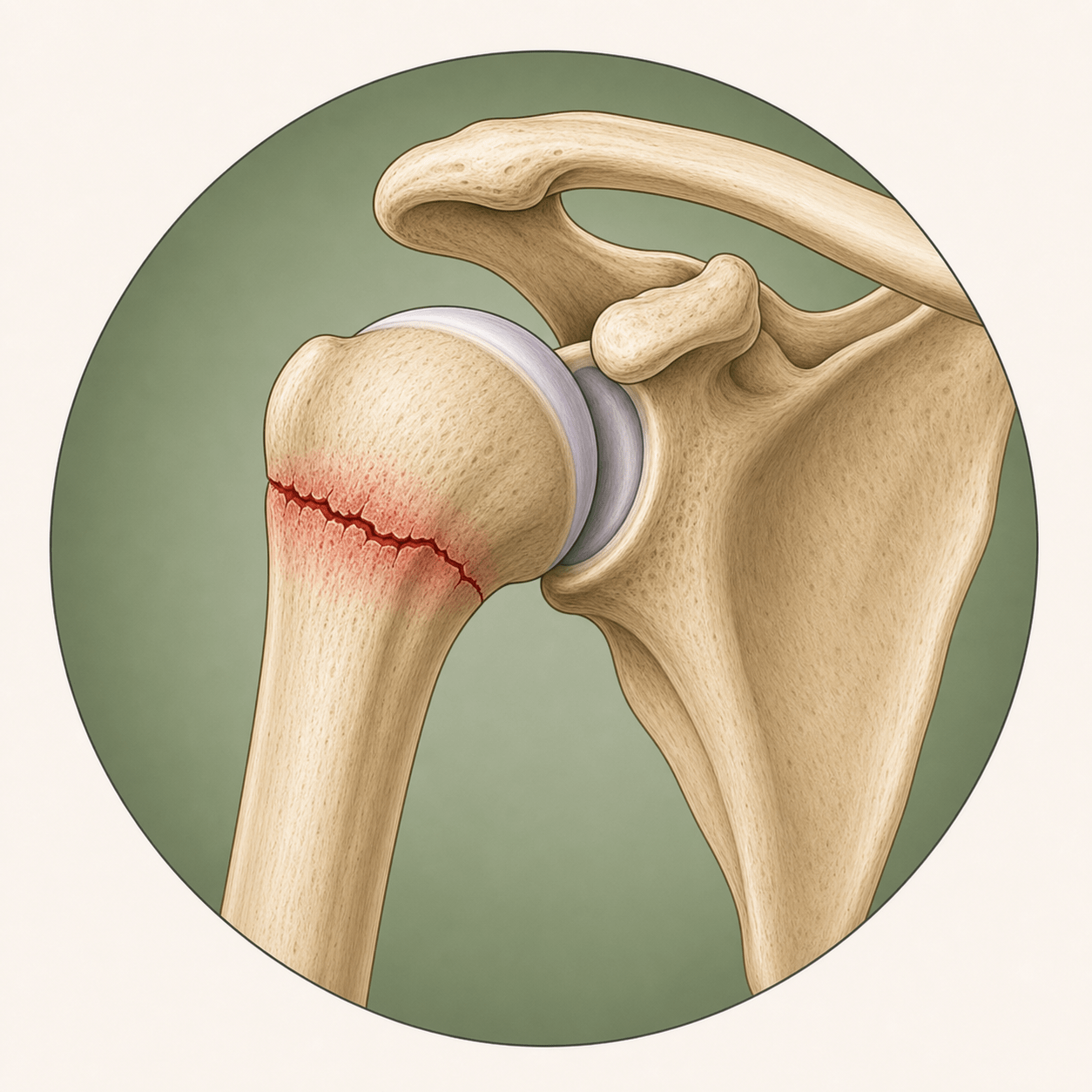 Shoulder
Can affect reaching, dressing, and sleep
Shoulder
Can affect reaching, dressing, and sleep
Nutrition for Bone Health
Bone health is not just about taking calcium. Bones need a broad foundation: enough calcium and vitamin D, adequate protein, potassium-rich foods, less excess sodium, and a balanced diet with fruits and vegetables.
Calcium
Food sources are preferred when possible. Many women over 50 need about 1,200 mg total per day from food plus supplements.
Vitamin D
Vitamin D supports calcium absorption. Some patients need a blood level checked and individualized dosing.
Protein
Protein supports muscle, balance, and fracture recovery. Low protein intake can increase fall risk.
Potassium note: Potassium-rich foods may support bone health, but people with kidney disease or certain medications should talk with a clinician before intentionally increasing potassium intake.
Exercise: Bones, Strength, and Balance
Exercise helps bones directly and lowers fracture risk by improving strength, balance, posture, and fall prevention. The most effective plan is usually more specific than walking alone.
- Progressive strength or resistance training at least 2 days per week
- Weight-bearing activity such as walking, stair climbing, dancing, or hiking
- Supervised impact or power training when appropriate for the patient's fracture risk and fitness level
- Balance training such as tai chi or heel-to-toe walking
- Posture and back-strengthening exercises
For patients who are appropriate for supervised higher-intensity training, Onero is an evidence-based program designed for bone health that combines resistance, impact, and balance work. In Santa Fe, Exercise Lab Santa Fe offers Onero-based training and can help patients work within an appropriate safety framework.
Safety First
People with severe osteoporosis, spine fractures, recent fractures, balance concerns, or significant pain should get individualized guidance before starting heavy resistance, jumping, or impact work. A clinician or physical therapist can help decide what is safe.
When Is Medication Recommended?
Medication may be recommended when fracture risk is high enough that nutrition and exercise alone are unlikely to provide enough protection.
- T-score of -2.5 or below at the spine, hip, or femoral neck
- Hip or spine fracture, regardless of T-score
- Osteopenia plus high fracture risk based on FRAX
Common FRAX thresholds include a 10-year major osteoporotic fracture risk of 20% or higher, or a 10-year hip fracture risk of 3% or higher.
Osteoporosis Medication Options
Osteoporosis medications generally fall into two groups. The best choice depends on fracture risk, kidney function, prior fractures, spine versus hip risk, cost, convenience, side effects, and patient preference.
Antiresorptive medications
These slow bone breakdown. Examples include bisphosphonates such as alendronate (Fosamax), risedronate (Actonel, Atelvia), ibandronate (Boniva), and zoledronic acid (Reclast); denosumab (Prolia); and raloxifene (Evista) for selected patients.
Bone-building medications
These help stimulate new bone formation and are generally used for people at very high fracture risk. Examples include teriparatide (Forteo), abaloparatide (Tymlos), and romosozumab (Evenity).
Osteoporosis Treatment Options Table
This table is meant to help patients understand the main options. It is not a prescribing chart, and the best choice depends on individual fracture risk and medical history.
| Treatment option | How given | Spine? | Hip? | Often considered when | Key caution |
|---|---|---|---|---|---|
| Alendronate (Fosamax) or risedronate (Actonel, Atelvia) | Pill, usually weekly | Yes | Yes | Common first-line options for many patients | Must be taken correctly to reduce esophagus/stomach irritation |
| Ibandronate (Boniva) | Monthly pill or IV every 3 months | Yes | Not proven | Spine-fracture risk is the main concern | Not usually preferred if hip-fracture prevention is a major goal |
| Zoledronic acid (Reclast) | IV infusion, usually yearly | Yes | Yes | Yearly dosing preferred / trouble tolerating oral bisphosphonates | Kidney function must be appropriate; flu-like symptoms can occur |
| Denosumab (Prolia) | Injection every 6 months | Yes | Yes | Strong antiresorptive therapy is needed and dosing can stay on schedule | Do not stop or delay without a transition plan |
| Raloxifene (Evista) | Daily pill | Yes | Not proven | Selected postmenopausal patients | Can increase blood clot risk and hot flashes |
| Teriparatide (Forteo) or abaloparatide (Tymlos) | Daily self-injection | Yes | Not proven | Very high spine-fracture risk or multiple fractures | Must be followed by antiresorptive medication |
| Romosozumab (Evenity) | Monthly injections for 1 year | Yes | Yes | Very high fracture risk when bone-building first is appropriate | Avoid with recent heart attack or stroke; follow with antiresorptive therapy |
Treatment Sequence Matters
Denosumab (Prolia) should not be stopped or significantly delayed without a plan. Stopping can cause rapid bone loss and a surge of spine fractures. Bone-building medications also need follow-up therapy to maintain gains.
What an In-Home Visit Can Help Clarify
Osteoporosis care is not just a scan result. A thoughtful visit can help clarify what your T-score means, whether FRAX should be calculated, whether labs are needed to look for secondary causes, whether medication is recommended, and how to build a realistic nutrition and exercise plan.
Santa Fe Mobile MD provides in-home, in-person care for patients who want careful, practical guidance about bone health, fracture prevention, and treatment options.
Frequently Asked Questions
What is the difference between osteopenia and osteoporosis?
Osteopenia means low bone mass, usually a T-score between -1.0 and -2.5. Osteoporosis means lower bone density, usually a T-score of -2.5 or below. Some people with osteopenia still need treatment if their fracture risk is high.
Is osteoporosis painful?
Osteoporosis itself usually does not cause pain until a fracture occurs. Spine fractures may cause back pain, height loss, or posture changes, but some spine fractures are found only on imaging.
Can diet and exercise reverse osteoporosis?
Nutrition and exercise are essential, but they may not be enough for people at high fracture risk. Many patients need medication to meaningfully reduce fracture risk.
Why is Prolia different from a bisphosphonate holiday?
Bisphosphonates stay in bone for a period of time after stopping. Denosumab (Prolia) does not. If denosumab is stopped or delayed without another medication, bone loss can happen quickly and spine fracture risk can rise.
What exercises should I avoid with osteoporosis?
People with severe osteoporosis, spine fractures, recent fractures, balance concerns, or significant pain should get individualized guidance before starting heavy resistance, jumping, or impact work. Many patients can still benefit from supervised strength, balance, and posture work.
Concerned About Bone Density or Osteoporosis?
If you have osteopenia, osteoporosis, a prior fracture, or questions about a DXA scan, schedule an in-home visit with Santa Fe Mobile MD to review your risk and discuss a practical plan.
This article is educational and does not determine whether osteoporosis medication is appropriate for an individual patient. Bone health decisions should be individualized based on fracture history, DXA results, FRAX risk, medical history, kidney function, medications, and patient preferences.